By: Jaine Roberts
Send to a friend
The details you provide on this page will not be used to send unsolicited email, and will not be sold to a 3rd party. See privacy policy.
TB is linked with a deadly silicosis epidemic hidden for decades in rural South Africa. Gold mining firms must make amends, says Jaine Roberts.
Across the rural Eastern Cape province in South Africa, up to half of men admitted to hospital with tuberculosis (TB) are former gold miners. This should not be surprising: the incidence of TB among miners is 2,000 cases per 100,000, four times the national incidence.
But researchers rarely ask about occupation when studying the distribution and determinants of illnesses such as TB — and the result here is a hidden epidemic of silicosis-related TB among former gold miners in South Africa.
SPEED READ
- South Africa's miners have four times the national incidence of TB
- Only recently has their respiratory health been studied
- The mining industry must lead the way to provide compensation and better healthcare
Silicosis is a serious lung disease caused by breathing in dust (formed during mining) that contains silica, a naturally occurring element. People with silicosis are particularly susceptible to TB.
It is poor epidemiology just to associate TB with HIV, while the epidemic of silicosis — an occupational lung disease for which sufferers bear no responsibility — is denied and hidden. This can also be seen as a convenient escape for the mining industry.
The stories of the miners need to be told.
Mining links missed
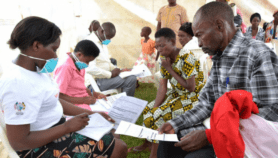
Thandile Qwalela died in 2009, aged 48, in a TB ward in a remote part of the Eastern Cape. He had worked for 17 years as an underground gold miner, was sent home with TB, and received no compensation or occupational health surveillance after leaving the mine.
His story is typical of many for decades, with no solution in sight. Half of the men in Qwalela's TB ward, at the time of his last admission, were migrant miners from the former black 'homelands' of apartheid South Africa. Their TB is diagnosed; their silicosis is not. A report I wrote in 2009 tells more of these tragic stories. [1]
For 70 years, no studies were done on the respiratory health of black miners. It was only in the mid-1990s that a group of dedicated occupational health researchers started the Libode study in the Eastern Cape. [2] At the same time, there was a second study on former miners who had returned to Botswana. [3]
These surveillance studies of pneumoconiosis (dust-related respiratory disease) found prevalence rates for silicosis of more than 30 per cent among former gold miners in Botswana, Lesotho and South Africa. The real prevalence could be higher, as those counted in the studies could be considered 'healthier' men who survived the disease.
No compensation
The epidemic of silicosis in South Africa is the legacy of an occupationally acquired disease that has been 'exported' or 'externalised' to the rural areas of the country.
Migrant labour systems established under apartheid, when workers from South Africa or neighbouring countries were given a pass to work away from their homelands, are still deeply entrenched in the country.
These systems return men too ill to work back to their homes, where they are reliant on primary healthcare clinics and district hospitals facing a shortage of doctors and x-ray services. This continues to this day, long into post-apartheid South Africa.
Tens of thousands have died without ever receiving — or even being aware of — the country's Benefit Medical Examination (BME) and the autopsies their families are entitled to under the Occupational Diseases in Mines and Works Act (ODMWA) of 1973.
Without medical examination (a chest x-ray or a simplified autopsy) there is no compensation — and the epidemic of silicosis in South Africa can be denied by the mining companies.
Industry focus on HIV
AngloGold Ashanti, one of the largest mining companies in the world, established a clinic in Lusikisiki, Eastern Cape, in the mid-1990s. It was well-equipped — a showcase for the provision of antiretrovirals (ARVs) and primary healthcare services.
But while many visitors were flown in to see that amining company was actively assisting state-run health services, silicosis was not addressed.
Lusikisiki has had the highest recruitment figures for miners from the Eastern Cape to serve the gold mining industry. Yet the clinic focused on HIV and the provision of ARVs. It did not offer one medical examination for silicosis.
It was left to an NGO with few resources, the Lusikisiki Community Development Programme, to help transport miners to the only silicosis service, at Mthatha General Hospital, itself established only last year, more than 100 kilometres from Lusikisiki.
Miners can be traced
The Employment Bureau of Africa (TEBA) is the recruitment arm of the mining industry. Employment records exist, and former migrant miners can be found in their home areas — if there is the will to do so.
This will has not existed at the Chamber of Mines and its member companies, despite commitment to corporate social responsibility, such as in AngloGold Ashanti's 2006 annual report, which acknowledged a legacy of silicosis within the labour-sending areas of South Africa. [4]
Miners who fall ill are still sent home to rely, in ignorance of their rights, on government-funded rural health services that are stretched to the limit. The conditions that maintain such widespread lack of awareness need to be addressed urgently. There is a need for ongoing medical surveillance of dust-related respiratory disease, with the appropriate compensation paid.
Mining companies need to face the evidence and offer redress, even so late in the day, to ensure that former miners are identified, diagnosed and compensated before they die.
The migrant labour system has hidden the epidemic of silicosis for decades. But the epidemiological evidence collected in the last 15 years is now sufficient to expose this "silent scourge", as the historian Shula Marks has described it.
The epidemic must stop being buried in rural areas of South Africa.
Jaine Roberts is director of research at Rhodes University in the Eastern Cape, South Africa. Her work as a public health researcher has focused on asbestos-related disease and the occupational disease compensation system for miners, and on silicosis and tuberculosis in gold miners. Roberts can be reached at [email protected]
References
[1] Roberts, J. The hidden epidemic amongst former miners: silicosis, tuberculosis and the Occupational Diseases in Mines and Works Act in the Eastern Cape, South Africa. (Health Systems Trust, 2009)
[2] Trapido, A.S. et al. Prevalence of occupational lung disease in a random sample of former mineworkers, Libode District, Eastern Cape Province, South Africa. America Journal of Industrial Medicine 34, 305–313 (1998)
[3] Steen, T.W. et al. Prevalence of occupational lung disease among Botswana men formerly employed in the South African mining industry. Occupational and Environmental Medicine 54, 19–26 (1997
[4] Legacy of silicosis. (AngloGold Ashanti Annual Report, 2006)
More on TB