20/07/21
‘Mass exodus’ of health staff to follow COVID-19

By: Fiona Broom, Laura Owings and Hazem Badr
Send to a friend
The details you provide on this page will not be used to send unsolicited email, and will not be sold to a 3rd party. See privacy policy.
Health worker deaths, migration and aid cuts put health systems at risk, warn global health security specialists.
Across the developing world, health and care workers are facing a similar scenario: the COVID-19 illnesses and deaths of colleagues, along with migration and resignations, are compounding workloads and stress for those still on the frontline.
The World Health Organization (WHO) says that “at least” 115,000 health and care workers have died from COVID-19, though director-general Tedros Adhanom Ghebreyesus acknowledges the true number is likely higher as data reporting is “scant”.
With COVID-19 spreading exponentially in Africa, and Latin America and Asia Pacific also facing unrelenting health emergencies, health worker deaths will likely continue to rise.
“Investing in women is the best investment we can make for all our futures and the future of health security.”
Roopa Dhatt, executive director Women in Global Health.
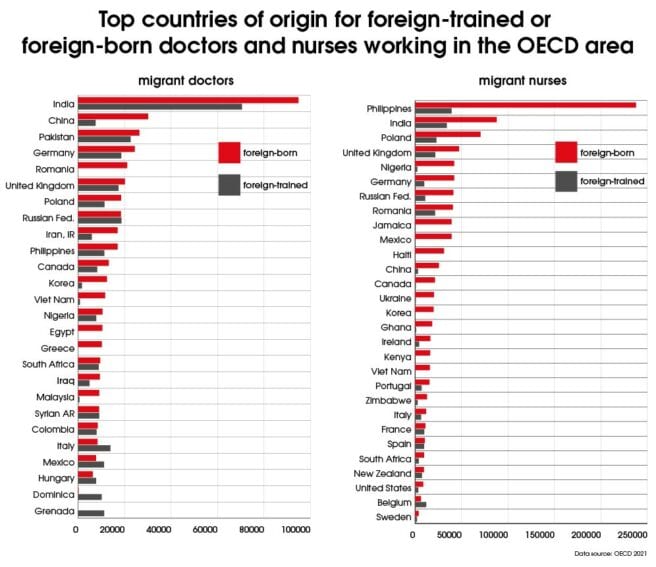
In the world’s wealthiest countries, the numbers of foreign-trained or foreign-born doctors and nurses have been on the increase for the past 20 years. Now, the loss of staff through death and migration is leaving knowledge gaps in already fragile health systems, say advocates and health workers.
But global health security specialists believe that amid the trauma of the pandemic lie opportunities to create policies that protect health staff and incentivise them to stay.
Protect and invest
“Health workers all over the world have put their lives on the line to try and keep people safe from COVID-19, yet far too many have been left unprotected and paid the ultimate price,” said Steve Cockburn, head of economic and social justice at Amnesty International. “For one health worker to die from COVID-19 every 30 minutes is both a tragedy and an injustice.”
For the women who make up about 70 per cent of health and care workers worldwide, this lack of security has meant using personal protective equipment designed for men — which often fails to protect women — as well as violence and harassment in the workplace.
Women in Global Health, an international network advocating for gender equality in global health leadership, has jointly launched what it calls “a new social contract for women in the health and care workforce”. The Gender Equal Health and Care Workforce Initiative, a partnership between the WHO, Women in Global Health and the government of France, aims to strengthen policy that will invest in, and protect, health and care workers.
“Health workers are exhausted, many want to leave. We cannot afford to lose one single worker at this time,” says Roopa Dhatt, an Indian physician and executive director of Women in Global Health. “Investing in women is the best investment we can make for all our futures and the future of health security.”
The world is reliant on women to deliver health and care services, Tedros told the Generation Equality Forum, where the first round of commitments to the Initiative was announced on 1 July.

Phumzile Mlambo-Ngcuka, UN Women executive director, opens the Generation Equality Forum in Paris. Governments, civil society and the private sector pledged US$40 billion to accelerate gender equality by 2026. Copyright: UNESCO/Christelle ALIX, (CC BY-NC-ND 2.0).
Women account for about 90 per cent of nurses and midwives, and close to half of all physicians, he said.
“This reliance demands that we ask ourselves tough questions on workplace conditions and equity, including how we value and reward women in the health and care workforce,” Tedros said. “And how we guarantee that workplaces are free from discrimination, violence, sexual exploitation and abuse.”
As governments — including Mexico, Pakistan, Democratic Republic of Congo, and Liberia — along with non-government organisations committed to the gender policy initiative, Dhatt said that millions of health and care workers were unpaid or underpaid and had no access to COVID-19 vaccines.
“We must provide incentives for women to stay,” says Dhatt.
Poaching staff
The global South has long supplied many of the human resources for health systems in the global North. And as health services in the United Kingdom, the US and Europe struggled under the weight of their respective COVID-19 crises, the demand for trained staff from the global South intensified.
Across the world’s wealthiest countries, nearly 25 per cent of all doctors and 16 per cent of nurses were born abroad, according to a briefing paper from the Organisation for Economic Co-operation and Development (OECD). The paper, published in May, examines how wealthy countries have sought to attract staff from developing countries in response to the COVID-19 pandemic.

The brief acknowledged that the countries from which staff were being enticed “were already facing severe shortages of skilled health workers before the COVID‑19 pandemic”.
As the UK launched a fast-track Health and Care Visa in 2020 to attract more foreign health workers, the government also drastically reduced its foreign aid budget — a move at odds with advice from the OECD.
Mitigating the factors that push health professionals to leave their home countries requires policy responses that “reinforce international co-operation, notably Overseas Development Assistance and technical assistance, to help less advanced countries build up a sufficient health workforce and to strengthen their health systems”, the OECD brief said.
Writing in The BMJ, Kaci Kennedy McDade and Wenhui Mao from Duke University’s Center for Policy Impact in Global Health said the aid cuts would put global health systems at risk. More than half of the 102 countries where aid has been cut are low- and lower-middle income and nearly a quarter are fragile or affected by conflict, they said.
Health worker deaths
In fragile health systems, the knowledge that is lost when a community health worker or a highly trained medical expert dies can have long-term impacts, say global health advocates.
The Philippines is the largest contributor of nurses to wealthy countries, OECD data shows. India provides the highest number of foreign doctors, and the second-highest number of migrant nurses.
The Filipino UK Nurses Association has raised concerns about the disproportionately high rate of deaths from COVID-19 among staff within the country’s National Health Service (NHS) and in social care. In the US, more than 30 per cent of the nurses who have died of COVID-19 were Filipinos, though they make up just four per cent of the country’s registered nurses, according to the National Nurses United union.
At home in the Philippines, prominent frontline health specialists have been lost to the pandemic. Paediatric surgeon Leandro Resurreccion III and Salvacion Gatchalian, who was president of the Philippine Pediatric Society and a paediatric infectious diseases expert, died in March 2020.
Gatchalian helped create the Philippines Coalition Against Tuberculosis and led a children’s tuberculosis initiative, while Resurreccion had returned from Australia to work for the Philippines’ health service.
Highly skilled researchers are scarce in low- and middle-income countries, says Glenda Gray, president of the South African Medical Research Council (SAMRC). She tells SciDev.Net: “Any loss of scientists either through death or migration is a concern.”

Research suggests physician migration costs poor countries almost US$16 billion annually and contributes to excess deaths resulting from lost medical knowledge.
With emigration rates of doctors and nurses as high as 50 per cent from some African and Latin American countries, according to the OECD, this can mean that more doctors born in these countries are working in the OECD area than in their countries of origin.
Africa’s research community lost a respected and loved colleague when renowned HIV scientist Gita Ramjee died of COVID-19-related complications in March 2020. Among a long list of roles that Ramjee played, she managed large-scale research networks with the SAMRC for more than 25 years.
“Gita was fundamental and inextricably linked to the endeavours to find solutions to prevent HIV in women. She was tireless in this pursuit, her tenacity will never be forgotten,” Gray said last year. Winnie Byanyima, executive director of UNAIDS, said Ramjee’s death was a huge loss “at a time when the world needs her most”.
Stemming the tide
Health workers in fragile systems face a vicious circle: poor pay and working conditions drive migration and pressure, and stress and workloads increase for the staff who remain. With COVID-19 has come the deaths of colleagues, and long-term physical and mental health effects.
“The post-COVID-19 phase will witness a mass flight of doctors as long as the situation remains as it is and the suffering continues.”
Al Arabi Bin Hara, Algerian doctor
“The psychological impact of deaths, infections and [increased workloads] prompted many doctors to request leave, and in the event of management refusal, some resorted to resigning from governmental hospitals,” Egyptian physician Abdel Hamid Mahmoud tells SciDev.Net.
Johan Fagan, an ear, nose and throat disease specialist at the University of Cape Town, says policies such as the UK’s fast-track Health and Care Visa will spur further migration.

“These countries aren’t training enough of their own healthcare professionals and are exploiting the workforce in developing countries,” Fagan says. “In a pandemic, this has a significant impact on our health systems and how we’re able to deliver care.”
Algerian doctor Al Arabi Bin Hara predicts an exodus of skilled workers once borders reopen. “Last year and the beginning of this year, there were the smallest number recorded in doctors’ immigration because of the closed borders as of the measures imposed by the pandemic,” Bin Hara says.
“The post-COVID-19 phase will witness a mass flight of doctors as long as the situation remains as it is and the suffering continues.” What hurts, says Bin Hara, is that hospitals and clinics in Europe — particularly in France — are attracting Algerian doctors with critical specialisations that are often lacking even in Algeria’s largest hospitals.
“We must invest now in nursing education, leadership, jobs and practice, and we need member states to own their new strategy and implement it now.”
Howard Catton, head of International Council of Nurses
In Zimbabwe, which has one of the highest emigration rates for home-trained doctors, experts are also sounding a warning. Charles Moyo, a Zimbabwean doctor training in South Africa, says Africa will face a healthcare crisis if the tide of health worker losses is not stemmed.
“The healthcare system is already strained by limited resources and by COVID-19. If more manpower is lost, the entire healthcare system could collapse,” he says.
The International Council of Nurses, which has signed on to support the Gender Equal Health and Care Workforce Initiative, celebrated the unanimous adoption at the World Health Assembly of the WHO’s updated global nursing and midwifery strategy. The strategy presents policy priorities to support midwives and nurses towards universal health coverage.
ICN chief Howard Catton said the strategy’s message was clear. “We must invest now in nursing education, leadership, jobs and practice, and we need member states to own their new strategy and implement it now,” Catton said.
“Of course, the tragic irony is that if we had done this before, we would have had a better protected healthcare workforce, and fewer of our colleagues would have died.”