
By: Neerja Chowdhary and Vijay Shankar
Send to a friend
The details you provide on this page will not be used to send unsolicited email, and will not be sold to a 3rd party. See privacy policy.
Mental disorders such as anxiety, depression and suicide attempts are a reality for the poor as much as they are for the rich, even though they are often overlooked. Data from the WHO’s Mental health atlas 2014 show that suicide rates can be very similar between countries as different in income status as Vietnam and the United Kingdom, with five and six suicides per 100,000 people, respectively. [1] But few people in the developing world get the mental healthcare they need, and many patients are treated inhumanely or offered treatments that do more harm than good.
Mental disorders and their causes
Mental illnesses include a range of conditions such as depression, generalised anxiety, panic attacks, bipolar disorder, schizophrenia and dementia (Figure 1).
Figure 1: Mental disorders
- Depression types
-
Depression: a condition with many symptoms that vary, but can include feeling tearful, restless, indecisive, despairing, isolated and irritable. Physical symptoms can include moving and speaking more slowly than usual, unexplained aches and pains, constipation and insomnia. Depression is described as mild, moderate or severe (clinical), depending on the impact it has on the person’s life — from feeling in low spirits, especially when faced with personal loss, to feeling persistently sad in a way that interferes with everyday life. There are specific forms of depression such as seasonal affective disorder and postnatal depression, and people who are severely depressed can have psychotic experiences and suicidal feelings.
Postnatal depression: a condition that usually develops within six weeks of giving birth, and should not be confused with the ‘baby blues’, which only lasts a few days and affects most mothers. Typical symptoms include feeling low, worthless, sad, tearful and guilty. Some mothers may feel hostile or indifferent to their baby or partner. The cause may be hormonal in combination with a lack of support, low self-esteem, poor living conditions and a history of mental health problems such as depression.
Seasonal affective disorder: a type of depression related to the amount of daylight available in different seasons. It differs from most people’s reactions to changes in seasons by how severely mood and energy levels are affected, and by the impact of symptoms on day-to-day life. For most people, it begins as the days become shorter in autumn and winter and starts to lift in spring and summer. The causes are still unclear.
- Eating and body image
-
Body dysmorphic disorder: an anxiety disorder related to body image. Someone with the disorder is anxious about an aspect of their appearance such as a facial feature or their weight, and may develop rigid routines and habits such as checking how they look or picking at their skin. They can also experience shame, guilt, loneliness, depression and, in severe cases, even self-harm and suicidal feelings.
Eating disorders: disorders that involve focusing on food as a distraction that helps people disguise painful feelings that are hard to face or resolve. Someone with bulimia nervosa tends to binge on large amounts of food in secret and then get rid of the food through vomiting or using laxatives. Someone with anorexia nervosa may dramatically reduce how much they eat, exercise compulsively and avoid high-calorie foods, and also use drugs to suppress appetite. Someone with binge eating disorder feels compelled to eat all the time, even when uncomfortably full. Eating disorders are associated with depression, self-esteem issues and anxiety.
- Mania
-
Bipolar disorder: a mood disorder previously called manic depression, which involves periods of feeling manic or ‘high’ (excited, euphoric, supremely confident and adventurous) and then feeling depressive or ‘low’ (tired, sluggish, listless and lacking in confidence). At times, a person can feel both high and low. The cause is still unknown, but likely factors include childhood trauma, stress, brain chemistry and genetics.
Hypomania and mania: conditions that describe periods where people may feel intensely happy and ‘high’, self-important, energetic and restless. Their minds may race, they may talk extremely quickly, be easily distracted and become disinhibited and aggressive. They are related to bipolar disorder. Hypomania is less severe than full mania.
Manic depression: see bipolar disorder.
- Personality disorder types
-
Borderline personality disorder: a disorder of mood and of how the person interacts with others. People with the condition may: worry about others abandoning them; experience very intense emotions that can change rapidly; and feel emotionally empty and angry. Making and keeping stable relationships may be difficult for them, and the sense of who they are can change according to who is around them. When stressed, they can experience paranoia and have psychotic experiences.
Personality disorders: conditions that cause people to have rigid patterns of feeling, thinking and behaving that make it harder for them to deal with everyday life. Psychiatrists have identified ten types of disorders in three groups. The ‘suspicious’ group includes antisocial personality disorder, where people are likely to act impulsively and behave dangerously with no sense of guilt. The ‘emotional and impulsive’ group includes borderline personality disorder. The ‘anxious’ group includes narcissistic personality disorder, where people have fragile self-esteem, tend to resent other’s successes and believe they are more deserving than others.
- Psychosis, hearing voices and schizophrenia
-
Hearing voices: a form of auditory hallucination where a person hears voices when no one is around them, or which others cannot hear. Some may hear just their name or a few words, while others hear a running commentary. Hearing voices when falling asleep (hypnagogic hallucinations) or waking up (hypnopompic hallucinations) is caused by the brain partly being in a dream state. Other causes range from lack of sleep to physical illnesses, drugs, bereavement, traumatic experiences, psychotic experiences, schizophrenia, bipolar disorder and depression.
Psychotic experiences: disorders in which people perceive or interpret things around them differently from others. One type is hallucinations, where people either experience things that aren’t there or see objects in a distorted way. They may hear voices or feel things such as insects crawling on their skin. Another type is delusions, where a person believes something that has no basis in fact — for example that they can bring people back from the dead. A paranoid delusion can be very frightening as the person believes they are in mortal danger. A third type is ‘flight of ideas’, where someone moves too quickly from thought to thought, making links that others can’t follow.
Schizoaffective disorder: a diagnosis applied to someone who has psychotic symptoms similar to schizophrenia and mood symptoms like someone with bipolar disorder. The symptoms they experience include hallucinations, delusions, hypomania and depression.
Schizophrenia: a diagnosis given to people who experience symptoms including hallucinations, delusions, hearing voices, difficulty concentrating, a desire to avoid people and feeling disconnected from emotions. It is caused by a combination of factors, including stressful life events, drug abuse and too much of a chemical called dopamine that carries messages between brain cells. There is also a genetic component.
Tardive dyskinesia: the medical term for sudden jerky movements that can be a side effect of some antipsychotic drugs. The movements are unusual and out of someone’s control. They can make sufferers very self-conscious and exacerbate anxiety.
- Sleep
-
Sleep problems: problems such as difficulty falling asleep or frequently waking up in the night lasting weeks, months or years and affecting day-to-day life. Among the most common are insomnia (where a person has difficulty falling asleep or getting back to sleep), oversleeping, nightmares, sleep paralysis (when a person wakes up in the night and cannot move or speak) and sleep walking. They can result from various factors including medication and physical or mental illness such as depression and bipolar disorder, anxiety and schizophrenia.
- Stress and anxiety
-
Anger: an emotional reaction that becomes a problem when it harms the person or those around them. Signs of anger include shouting and being physically violent or verbally abusive. It can also be ‘passive aggressive’, where someone might ignore or be sarcastic to others, and it can be ‘inwardly aggressive’, where someone self-harms or experiences self-loathing. Anger can be a sign of a personality disorder or paranoia and it can also contribute to depression, anxiety and eating problems.
Anxiety: a normal emotion when faced with a stressful event or decision, which becomes a problem if a person feels anxious all the time, or if they feel overwhelmed. It includes feeling tense, uneasy, worried and fearful. Potential causes vary widely, from childhood experiences to a genetic disposition. Anxiety is a major factor in a number of disorders: body dysmorphic disorder, generalised anxiety disorder, panic attacks, obsessive-compulsive disorder, phobias and post-traumatic stress disorder.
Generalised anxiety disorder: a broad anxiety diagnosis given to people who constantly feel anxious and fearful with no specific cause.
Panic attacks: extreme versions of the body’s reaction to stress and fear. A person having a panic attack may experience a pounding heartbeat, nausea and chest pains, have difficulty breathing and may feel faint or afraid they are about to die. Episodes can last from five to 20 minutes and can be very frightening. Anxiety and post-traumatic stress disorder can result in panic attacks.
- Suicide and self harm
-
Self-harm: a set of behaviours that can take many forms, from cutting or poisoning yourself to hair pulling, overexercising, overdosing and eating disorders. It is a way of finding release from difficult feelings. Some say it gives them a sense of control, or that it conveys severe distress and even suicidal feelings to others. The causes can include pressure from school or work, worries about bullying, abuse, difficult feelings linked to another mental health problem, or depression, anxiety and anger.
Suicidal feelings: a sense of not wanting to go on living. A person with suicidal feelings is likely to feel overwhelmed by unbearable feelings and painful experiences, and may see no solution other than seeking ‘nothingness’. The feelings may result from a long list of factors that includes isolation and loneliness, the breakup of a relationship, bullying, debt, physical conditions and mental health problems such as depression, borderline personality disorder, schizophrenia and bipolar disorder.
- Other
-
Autism: a developmental disorder often not considered a mental health problem on its own, but it can be associated with a mental disorder such as anxiety or depression. Most people with autism have problems with social interaction, communication and language, as well as a narrow range of thoughts, interests and activities that are carried out repetitively. These make everyday life confusing and even frightening. Some people with autism may also experience problems with sensitivity to their senses.
Dementia: a condition linked with the ongoing decline of the brain beyond normal ageing. People with dementia may have problems with memory loss, language, understanding and judgement. These are usually accompanied by apathy, difficulty controlling emotions or poor motivation. Symptoms may also include depression and changes in mood or personality. Dementia is caused by disease or injury. Examples include Alzheimer’s disease, caused by the build-up of abnormal proteins in the brain, or stroke, which rapidly kills cells by inhibiting blood supply to the brain.
Dissociative disorders: conditions that change a person’s sense of reality beyond normal, brief periods of being ‘disconnected’. They are often linked with traumatic experiences. People with a dissociative disorder can end up with memory loss or feeling that their body is unreal. There are several types: in dissociative amnesia, a person forgets important incidents or personal information; in depersonalisation disorder, a person feels detached from their body; in dissociative fugue, someone can travel to a new location and assume a new identity; and in dissociative identity disorder, a person experiences shifts of identity as separate personalities.
Loneliness: an unmet need for rewarding social contact and relationships. It is not the same as being alone — many people are content with their own company. Circumstances such as retirement or moving to a new area can cause loneliness, but some people feel lonely regardless of their situation. They may consider themselves unlikeable and lack confidence, isolating themselves from other people. Conditions such as depression, anxiety, panic attacks or a phobia can contribute to feeling lonely, and vice versa.
Obsessive-compulsive disorder: an anxiety disorder where people have constant worrying thoughts that dominate their thinking. They might worry about harming themselves or others, for example, or obsess about infection and disease. To manage their obsessive thoughts, they develop compulsions. A person who worries about germs, for example, may develop handwashing rituals that they repeat many times a day.
Paranoia: a condition in which people have fears and thoughts that are greatly exaggerated and unfounded. Common paranoias include people feeling at risk of psychological harm (someone spreading rumours about them or bullying them), physical harm (someone wants to hurt them) or financial harm (someone is stealing from them). If the paranoia is part of a psychotic disorder, a person may also be hearing voices, which can compound the problem. Factors that can cause the condition include stressful life events, anxiety and depression, lack of sleep, physical illness and drugs and alcohol.
Phobias: extreme fears triggered by otherwise harmless objects, situations or events. They differ from everyday fears as they last for more than six months and have a major impact on a person’s life. Phobias can be specific, such as fear of animals, heights, tunnels or injections. They can also be more complex, such as fear of social situations or open spaces. Someone with a phobia has intense anxiety, physical symptoms such as dizziness and sweating, and may even experience panic attacks.
Post-traumatic stress disorder (PTSD): an anxiety disorder following a traumatic event such as war, road traffic accident, assault or natural disaster. While it is normal to feel distressed after witnessing such incidents, in PTSD the symptoms last for longer than a month and are very extreme. Symptoms include nightmares, distressing thoughts and flashbacks in which people relive the trauma, as well as physical symptoms such as insomnia, sweating and trembling.
Self-esteem: a phrase that describes beliefs that people have about themselves, their abilities and expectations. Those with poor self-esteem tend to focus on mistakes they’ve made and their weaknesses. Factors that can contribute to poor self-esteem include depression and anxiety as well as stress, poor relationships with people, loneliness, bullying in childhood and difficult life events such as bereavement.
Age-related conditions such as dementia, Parkinson’s and Alzheimer’s diseases are also included in mental disorders.
The impact of conflicts and natural disasters on mental health is important to note given recent or long-term crises that continue to affect millions around the world. For example, estimates suggest that more than two million Syrians are suffering from mild to moderate mental disorders. In Sri Lanka, where the effect of internal conflicts lasting more than 25 years were compounded by the 2004 tsunami, anxiety, depression and post-traumatic stress disorder have affected many. [2] Similarly, more than 20,000 people in Haiti sought care for psychosocial needs within 18 months of the major earthquake that hit the country in 2010. Nepal faced a devastating earthquake in April 2015, and as of May 2015 at least five per cent of people affected were at risk of suffering from mental health issues. The WHO estimates that humanitarian emergencies lead to mental disorders in five to ten per cent of the affected population.
Another important determinant of mental illness is violence in its many forms such as sexual abuse, trafficking and domestic violence by partners, more often inflicted upon children and women. A meta-analysis of studies on women exposed to intimate partner violence found post-traumatic stress disorder in more than 60 per cent of the women, depression in nearly half, suicidal thoughts and alcohol abuse in nearly a fifth, and drug abuse in about nine per cent. [3]
Social factors such as vulnerability to poverty can also influence the risk of mental illness. Studies from low- and middle-income countries (LMICs) reveal a significant association between depression and poverty indicators such as limited education, low income, lack of employment and housing difficulties. [4]
Although mental disorders can affect anyone regardless of age or gender, some problems are gender specific, such as the onset of depression in women during or after childbirth. According to a 2012 systematic review, about ten per cent of pregnant women and 13 per cent of those who have recently given birth in LMICs suffer from anxiety and depression. [5]
Similarly, some mental illnesses are linked to advanced age. Mental health risks for the elderly are often associated with brain-related diseases such as dementia, Parkinson’s and Alzheimer’s diseases, along with familial and social neglect and loneliness. In developing countries, about 15 per cent of the over 60s suffer from a mental disorder. The number of people living with dementia worldwide is forecast to increase from 47.5 million currently to 135.5 million in 2050, most of them people living in LMICs, according to the WHO.
Shorter lives, poorer health and other impacts
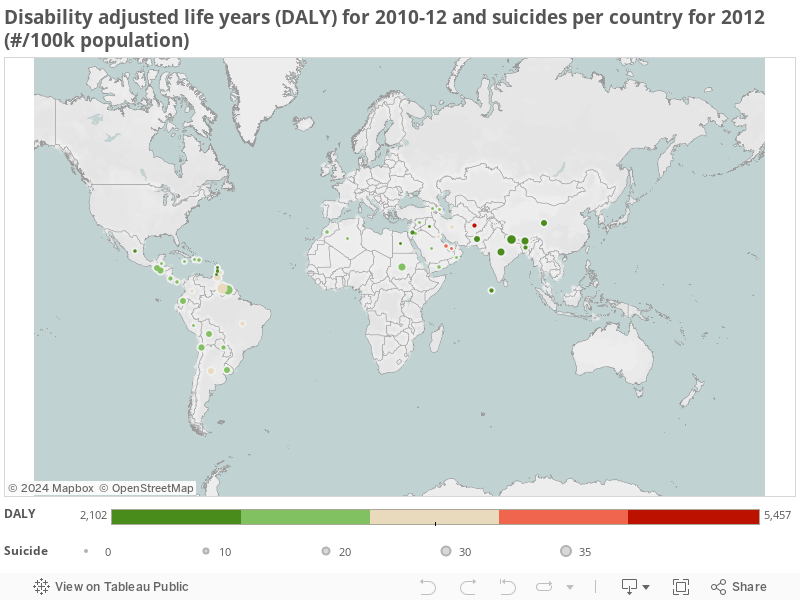
Mental disorders account for 13 per cent of the total global burden of disease (see figure 2). [6] Depression is the third leading contributor to this burden, according to 2011 estimates: an estimated 13 per cent of suicides are by people who suffer from depression, and people with depression are 20 times more likely to kill themselves than those who are not depressed. [7]
Suicide is a major contributor to the number of deaths across all ages worldwide. Nearly 900,000 people take their own lives each year and, this is expected to rise to 1.5 million deaths by 2020. [8] While getting accurate information on suicide is difficult in the global South because of political, cultural and religious hurdles, the WHO’s first global report on suicide prevention suggests that three-quarters of suicides occur in LMICs. [9]
The Million Death Study conducted in India shows how important suicide is in some LMICs: the country’s suicide rates are among the highest in the world (see figure 2). The study’s estimates for 2010 show that about three per cent of all deaths of those aged 15 or over were due to suicide, and that 40-50 per cent of suicides were by people aged between 15 and 29, with women more affected than men.
Figure 2
Apart from suicide, there are several other reasons for deaths due to mental illness. [10] Mental disorders increase the risk of substance abuse such as heavy smoking and drinking too much alcohol, as well as unhealthy eating habits. And these can lead to other health problems such as liver cirrhosis. In some cases, lifestyle and mental illness combine to raise the risk for other conditions. For example, people with schizophrenia who abuse alcohol are likely to engage in more risky sexual behaviour, increasing their risk of contracting sexually transmitted diseases such as HIV/AIDS.
Overall, mental illness can dramatically shorten life expectancy. In a 20-year study in South India of people with schizophrenia, the average age at death was about 34 years compared with a national average of just over 60 years. [11]
And the severity of the impacts, including social exclusion, varies depending on age and the type of the problem. [12]
Mental illness also has significant economic costs. [12] The World Economic Forum estimated that productivity losses in low-income countries due to mental illness cost US$200 billion in 2010, with this set to double by 2030. [15] Yet these countries invest a meagre 0.5 per cent of their total health spending on mental health, compared with 2.4 per cent in middle-income countries and 5.1 per cent in high-income ones.
Stigma and other hurdles to care
Despite the huge burden of mental illness and proven efficacy of certain treatments in LMICs, only one in five people with severe mental disorders in these countries receives treatment. [16] Experts call this the ‘treatment gap’. [17]
Treatment for mental disorders has received little policy focus in the developing world. According to the WHO’s Mental health atlas 2014, only 60 per cent of the surveyed 171 countries reported data on or evidence of all of the following: a relevant policy or action plan; relevant laws; programmes to promote mental health and prevent mental disorders; and mental health services and dedicated workforce. [1] The record is poorer when it comes to action plans: only about 15 per cent of countries have a fully implemented plan, 14 per cent have an unimplemented plan and ten per cent have no plan at all.
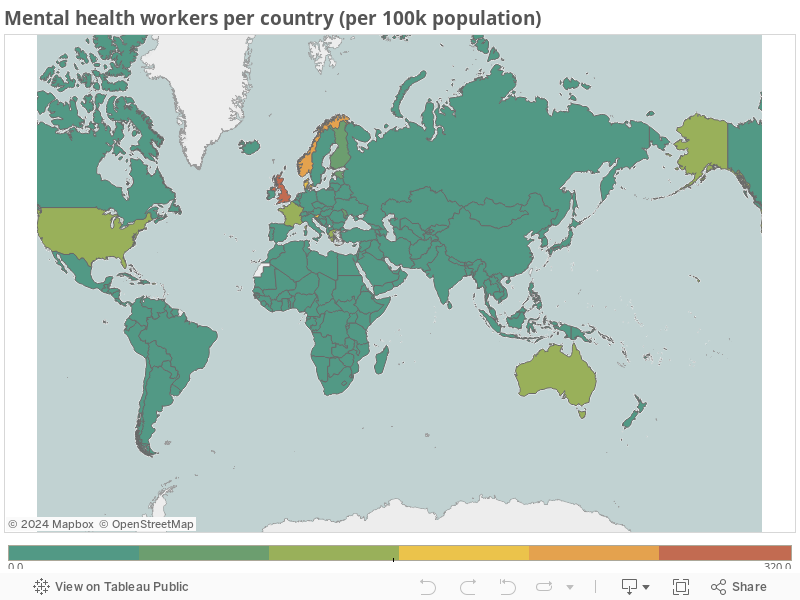
There is also a limited supply of resources: psychiatrists, nurses, care workers, hospital beds and other facilities. [18] On average, low-income countries have less than five psychiatrists for every million people — at least 10 times lower than high-income countries — and the difference in the rate of psychiatric nurses is much higher. [1] These figures show the huge inequalities in how skilled human resources for mental health are distributed across the world (see figure 2). Sierra Leone, for example, which endured civil conflict for years and more recently a deadly Ebola outbreak, has only one psychiatrist serving the entire country. And in India there is only one mental health worker for every 100,000 people despite a high national suicide rate of about 21 per 100,000 people.
Figure 3
Beyond the limited workforce and investments in mental healthcare, people in developing countries have another barrier to care: the high prevalence of stigma that often surrounds mental illness (See box 1). Stigma and social exclusion deter people from seeking help, delaying both the start of appropriate treatment and their recovery. Eventually, an emotionally and socially withdrawn person is likely to lose the opportunity to live a full and productive life. [19]
Box 1:Mental health and stigma |
|
In many countries — but perhaps more so in the global South — a mentally ill person is at risk of social stigma, discrimination or social exclusion that limits work opportunities. This affects both people’s livelihoods and a country’s productivity, translating to a high social and economic cost. In developing countries, where many people live in poverty and earn a living through informal work on a day-to-day basis, such discrimination and exclusion can severely affect their lives. And because of high healthcare costs and the need for multiple consultations, people on the poverty line either miss out on essential care or get pushed further into poverty.
Experts believe stigma arises for three reasons. [20] First is a lack of scientific knowledge about mental health among the public or misleading information spread by sham doctors, leading to false beliefs about mental illness being associated with sin or supernatural causes. Second are negative attitudes and prejudices that people might hold, so excluding or discriminating against patients. Finally, patients themselves often stigmatise themselves by internalising negative attitudes, and this can feed into their mental illness. |
Studies point to differences in stigma among cultural groups. For example, in much of Africa this is a silent epidemic — people with mental illness are hidden from their communities. [21] The stigmatisation of mental illness can be influenced by other factors, which are in turn strongly influenced by culture. The perceived cause of the illness is one example: in one study, the belief that mental illness has a genetic origin led Chinese Americans and European Americans to make different judgements about marriage and reproduction. [22] Beyond stigma, culture influences mental illness in diverse ways, for example in how people describe or name clinical syndromes or accept treatments.
Promising evidence-based strategies
Efforts to reduce the mental health treatment gap face many barriers. So innovative strategies are crucial to overcome them. Some programmes have attempted to do this by integrating mental health in primary care services, which makes care for mental illnesses more accessible and affordable. Another approach is to train lay or community health workers to deliver mental health treatments. This gets around the barriers of having enough human resources. Yet another approach is to adapt treatments in a systematic way to tackle stigma and other considerations that relate to the social environment, to address the acceptability barrier.
Non-specialist health workers with no mental health background have proved they can provide treatment effectively after a relatively short period of training and with continuing supervision. [23] One such example comes from Pakistan. Funded by research charity the Wellcome Trust, the experiment has proved that such an intervention can be integrated into healthcare systems where mental healthcare workforce or resources are limited. [24] And in Uganda, the Heartsounds programme has trained ‘peer-support workers’ to help people who have used mental health services in Kampala after they have returned to their homes, helping to fight the stigma and discrimination often linked to getting help.
This model could also work in humanitarian settings such as during or after conflicts. A recent study from Sri Lanka has suggested this possibility. [25]
Making services culturally sensitive is an important step towards making them more accessible, and the cultural barriers to seeking help call for non-traditional methods of treatment that people might be more likely to accept. [26] Psychiatrist Vikram Patel has argued that Western-style models of mental healthcare need to be adapted for low-income countries also because resources are in short supply. Culturally adapting mental health services is difficult and has had mixed results, but a framework for culturally sensitive psychosocial interventions published a decade ago has been used widely. [27,28]
Tech support
Beyond community-based care, modern mental healthcare can also take advantage of technology such as mobile phones and teleconferencing to provide personalised or individualised care.
Although mobile phone use in developing countries continues to rise, experts argue that the potential of mobile-based health interventions (or mHealth) has yet to be fully realised for mental health. [29] Technological tools tend to be underused in developing countries: only last year, a systematic review of programmes that use the internet to provide mental healthcare in LMICs found too little evidence to draw conclusions. [30] But a programme designed to help care for children with developmental disorders in rural Pakistan shows how information and mobile phone technology can be used to train their families to offer support (see Box 2). And a study among low-income people in the United States shows that text messaging can complement therapy for depression, helping to track patients’ thought patterns, activities and general wellbeing. [31]
Box 2: Support through mobile phone technology in Pakistan |
|
In 2012, Pakistan’s Human Development Research Foundation (HDRF) set up Family Networks for Kids, a three-year programme designed to use information and mobile phone technology to build and sustain family networks that support children with developmental disorders in a rural population of 30,000 people. Children with autism also often suffer from mental illnesses such as anxiety or depression. Most are left untreated either because families are unaware of the need to care for them, because health services are hard to reach or because of stigma.
The programme recruited and trained family members as ‘champions’ to lead on helping children in their own family and a network of up to seven other families. They worked to reduce stigma, share the care of children with community health workers, assist other champions and support other services catering for the children to maximise their impact. To begin with, technological tools were used to both help identify children in need and train family members to care for them. Family members were able to ring a mobile phone-based interactive voice system that guides them through questions to help identify whether their child may have a developmental disorder. The system helps overcome an important barrier to care in rural areas: the need to travel to a doctor or wait for a health worker to visit. It also slashed the cost of screening each child from US$7 to US$0.07 simply by eliminating the need for a door-to-door survey. Champions received training in evidence-based interventions using a tablet-based system with interactive, storytelling avatars and learning modules based on the WHO’s Mental Health Gap Action Plan (mhGAP). They used this technology to also train others in their part of the network. Although it was challenging to keep the volunteers motivated throughout the programme, there were positive results. In a recent evaluation, the project leaders report that the phone system correctly identified 84 per cent of under tens with developmental disorders. [32] There was also a fall in stigma and improvements in clinical measures such as children’s communication, mobility or ability to care for themselves. |
There may be another advantage to using mobile phones for mental healthcare: because many people see smartphones as a status symbol, care workers could use them to tackle the stigma of mental illness. [29] This can be done both by encouraging patients to use them to access services, and by associating treatment with the devices as a way to change social attitudes to mental health.
More revolutionary ways of using technology to treat mental illness are under development. [33] They include virtual reality therapy, computer-based methods and video games for paramedics, care providers or patients.
The way forward
Providing care for mental disorders is challenging in any part of the world. Initiatives such as mhGAP by the WHO aim to mitigate the mental health crisis in the developing world or resource-limited settings such as conflict areas. It is also crucial to boost training for health professionals, and promote more open acceptance of mental disorders and to tackle stigma against people with mental illness. Initiatives such as the WHO’s QualityRights project, which promotes human rights and better quality care for mental health patients, grabbed the attention of public figures such as film producer Gary Foster and author Gregory David Roberts — a potent way to make progress towards a better quality of life for millions of people with mental disorders in the developing world.
Neerja Chowdhary is a psychiatrist based in India (formerly global mental health coordinator at International Medical Corps), and Vijay Shankar is a freelance journalist based in the United Kingdom. Chowdhary can be contacted at [email protected] and Shankar at [email protected]
This article is part of our Spotlight on Mental health matters.
More on Health











